";s:4:"text";s:15692:"If you can't submit a request via telephone, please use our general request form or one of the state specific forms below .
EVKEEZA (evinacumab-dgnb)
RECORLEV (levoketoconazole)
STELARA (ustekinumab)
these guidelines may not apply. AYVAKIT (avapritinib)
endobj
CARVYKTI (ciltacabtagene autoleucel)
INBRIJA (levodopa)
Wegovy (semaglutide) injection 2.4 mg is indicated as an adjunct to a reduced calorie diet and increased physical activity for chronic weight management in adults with an initial body mass index (BMI) of 30 kg/m 2 (obesity) or 27 kg/m 2 (overweight) in the presence of at least one weight-related comorbid condition (e.g., hypertension, type 2 diabetes mellitus, or . Wegovy is only approved for use in people with a body mass index (BMI) of 30 or greater or in people with a BMI of 27 or greater who also have a metabolic health condition, like type 2 diabetes, high cholesterol, or high blood pressure . License to use CPT for any use not authorized herein must be obtained through the American Medical Association, CPT Intellectual Property Services, 515 N. State Street, Chicago, Illinois 60610. WebIf yes to question 1 and the request is for Contrave/Wegovy, has the patient lost at least 5% of baseline body weight or has the patient continued to maintain their initial 5% weight loss? Wegovy is indicated for use in: Adults: Obese ( BMI of 30 kg/m2 or greater) Overweight (BMI of 27 kg/m2 or greater) and have medical problems (e.g.high blood pressure, type 2 diabetes, or high cholesterol) due to your weight. BAVENCIO (avelumab)
ALIQOPA (copanlisib)
your Dashboard to submit your PA request. 0000054934 00000 n
The five character codes included in the Aetna Clinical Policy Bulletins (CPBs) are obtained from Current Procedural Terminology (CPT), copyright 2015 by the American Medical Association (AMA). General Exception Request Form (Self Administered Drugs) - (used for requests that do not have a specific form below, or may be used to request an exception) Open a PDF. 0000002222 00000 n
- 30 kg/m (obesity), or. 0000151642 00000 n
This approval process is called prior authorization. Drug list/Formulary inclusion does not infer a drug is a covered benefit. 0000011178 00000 n
endstream
endobj
startxref
FDA Approved Indication(s) Wegovy is indicated as an adjunct to a reduced-calorie diet and 0000045046 00000 n
increase WEGOVY to the maintenance 2.4 mg once weekly. Please contact CVS/Caremark at 855-582-2022 with questions regarding the prior authorization process. authorization (PA) guidelines* to encompass assessment of drug indications, set guideline SPRAVATO (esketamine)
You are now being directed to the CVS Health site. XIAFLEX (collagenase clostridium histolyticum)
Aetna has reached these conclusions based upon a review of currently available clinical information (including clinical outcome studies in the peer-reviewed published medical literature, regulatory status of the technology, evidence-based guidelines of public health and health research agencies, evidence-based guidelines and positions of leading national health professional organizations, views of physicians practicing in relevant clinical areas, and other relevant factors). 0000120040 00000 n
0000045019 00000 n
Drug Prior Authorization Request Forms. When required, request prior authorization through our vendor, Carelon (formerly AIM Specialty Health). 0000016896 00000 n
AYVAKIT (avapritinib)
endobj
CARVYKTI (ciltacabtagene autoleucel)
INBRIJA (levodopa)
Wegovy (semaglutide) injection 2.4 mg is indicated as an adjunct to a reduced calorie diet and increased physical activity for chronic weight management in adults with an initial body mass index (BMI) of 30 kg/m 2 (obesity) or 27 kg/m 2 (overweight) in the presence of at least one weight-related comorbid condition (e.g., hypertension, type 2 diabetes mellitus, or . Discard the Wegovy pen after use. 0000055600 00000 n
ADBRY (tralokinumab-ldrm)
VERZENIO (abemaciclib)
GAVRETO (pralsetinib)
Inpatient admissions, services and procedures received on an outpatient basis, such as in a doctor's office,
ZTALMY (ganaxolone suspension)
XPOVIO (selinexor)
EMFLAZA (deflazacort)
BALVERSA (erdafitinib)
HARVONI (sofosbuvir/ledipasvir)
B"_?jB+K DAkM5Zq\!rmLlIyn1vH _`a8,hks\Bsr\\MnNLs4d.mp
#.&*WS
oc>fv
9N58[lF)&9`yE
{nW Y &R\qe 0000054934 00000 n
VONVENDI (von willebrand factor, recombinant)
CAMZYOS (mavacamten)
These clinical guidelines are frequently reviewed and updated to reflect best practices. VIEKIRA PAK (ombitasvir, paritaprevir, ritonavir, and dasabuvir)
SYNRIBO (omacetaxine mepesuccinate)
MONJUVI (tafasitamab-cxix)
Providers may request a step therapy exception to skip the step therapy process and receive the Tier 2 or higher drug immediately. ILUVIEN (fluocinolone acetonide)
XIFAXAN (rifaximin)
P
JYNARQUE (tolvaptan)
There should also be a book you can download that will show you the pre-authorization criteria, if that is required. Wegovy (semaglutide) injection 2.4 mg is indicated as an adjunct to a reduced calorie diet and increased physical activity for chronic weight management Coverage Duration: Initial and Reauthorization: 6 months Authorization is not covered for the following: This is a listing of all of the drugs covered by MassHealth. Wegovy is covered, starting in 2022, with a PA. You can use the discount card, comes out to $24.99/month for me (Im on 1.7mg). Treating providers are solely responsible for medical advice and treatment of members. 0000069922 00000 n
ORACEA (doxycycline delayed-release capsule)
Disclaimer of Warranties and Liabilities. NAYZILAM (midazolam nasal spray)
ONPATTRO (patisiran for intravenous infusion)
All services deemed "never effective" are excluded from coverage. 0000180744 00000 n
WebWelcome. It would definitely be a good idea for your doctor to document that you have made attempts to lose weight, as this is one of the main criteria. 0000180332 00000 n
hb```b``mf`c`[ @Q{9
P@`mOU.Iad2J1&@ZX\2 6ttt
`D> `g`QJ@ gg`apc7t3N``X tgD?>H7X570}``^ 0C7|^ '2000 G>
Trulicity will approve for a diagnosis of type 2 diabetes 118 0 obj
<>
endobj
xref
0000008389 00000 n
[Document the weight prior to Wegovy therapy and the weight after Wegovy therapy, including the date the weights were taken:_____] Yes No 3 Does the patient have a body mass index (BMI) greater than or equal to 30 kilogram per . 0000179791 00000 n
0000043471 00000 n
0000055627 00000 n
WebSemaglutide (Wegovy) is a glucagon-like peptide-1 (GLP-1) receptor agonist. %%EOF
WebPrior Authorization tools are comprised of objective criteria that are based on sound clinical evidence. 0000045880 00000 n
OhV\0045| D
RHOFADE (oxymetazoline)
0000055627 00000 n
Enjoy an enhanced health care service and shopping experience with CVS HealthHUB in select CVS Pharmacy locations. 0000054864 00000 n
Alexander County, Illinois Land For Sale, 0000004021 00000 n
RYLAZE (asparaginase erwinia chrysanthemi [recombinant]-rywn)
AKYNZEO (fosnetupitant/palonosetron)
[emailprotected]\wbm"/,>it]xJi/[emailprotected]:'Yu]@[emailprotected]'}VoRgcxBu'abo*vn%H8Ldnk00X ya"3M TM y-$\6mWE y-.ul6kaR The prior authorization includes a list of criteria that includes: Individual has attempted to lose weight through a formalized weight management program (hypocaloric diet, exercise, and behavior modification) for at least 6 months prior to requests for drug therapy. The recently passed Prior Authorization Reform Act is helping us make our services even better. 0000002808 00000 n
Fax complete signed and dated forms to CVS/Caremark at 888-836-0730.
JUBLIA (efinaconazole)
BESPONSA (inotuzumab ozogamicin IV)
t
DORYX (doxycycline hyclate)
EUCRISA (crisaborole)
T
In addition, coverage may be mandated by applicable legal requirements of a State or the Federal government. 0000042653 00000 n
0000002222 00000 n
0000055177 00000 n
VIZIMPRO (dacomitinib)
BREXAFEMME (ibrexafungerp)
Octreotide Acetate (Bynfezia Pen, Mycapssa, Sandostatin, Sandostatin LAR Depot)
<>/Metadata 133 0 R/ViewerPreferences 134 0 R>>
BRUKINSA (zanubrutinib)
Explore differences between MinuteClinic and HealthHUB. Copyright 2023
RITUXAN (rituximab)
ERLEADA (apalutamide)
If you need any assistance or have questions about the drug authorization forms please contact the Optima Health Pharmacy team by calling 800-229-5522. 0000029629 00000 n
Drug Prior Authorization Request Forms Vabysmo (faricimab-svoa) Open a PDF Viscosupplementation with Hyaluronic Acid - For Osteoarthritis of the Knee (Durolane, Gel-One, Gelsyn-3, Genvisc 850, Hyalgan, Hymovis, Monovisc, Orthovisc, Supartz FX, Synojoynt, Triluron, TriVisc, Visco-3) Open a PDF An exception can be requested following a denial of a prior authorization or can be submitted at the onset of the request. ),)W!lD,NrJXB^9L 6ZMb>L+U8x[_a(Yw k6>HWlf>0l//l\pvy]}{&K`%&CKq&/[a4dKmWZvH(R\qaU %8d
Hj @`H2i7(
CN57+m:#94@.U]\i.I/)"G"tf
-5 0YjjB \K2z[tV7&v7HiRmHd 91%^X$Kw/$ zqz{i,vntGheOm3|~Z ?IFB8H`|b"X ^o3ld'CVLhM >NQ/{M^$dPR4,I1L@TO4enK-sq}&f6y{+QFXY}Z?zF%bYytm. hb```}\B ce`a87FIsVf):t8Ip.HgDGGGYf R np00%X Bevacizumab
AMONDYS 45 (casimersen)
Wegovy This fax machine is located in a secure location as required by HIPAA regulations. %PDF-1.6
%
! Didnt have to call Aetna to ensure it would be that cost, it just is. See multiple tabs of linked spreadsheet for Select, Premium & UM Changes. EMGALITY (galcanezumab-gnlm)
How to access the OptumRx PA guidelines: Reference the OptumRx electronic prior authorization ( ePA ) and (fax ) forms. 0000001751 00000 n
0000044887 00000 n
0000002627 00000 n
0000002756 00000 n
You, your appointed representative or your prescriber can request prior authorization by calling Express Scripts Medicare toll free at 1.844.374.7377, 24 hours a day, 7 days a week. SEGLENTIS (celecoxib/tramadol)
DIFFERIN (adapalene)
0000002527 00000 n
TABRECTA (capmatinib)
NEXLIZET (bempedoic acid and ezetimibe)
Patient Information Low Molecular Weight Heparins (LMWH) - FRAGMIN (dalteparin), INNOHEP (tinzaparin), LOVENOX (enoxaparin), ARIXTRA (fondaparinux)
You can review prior authorization criteria for Releuko for oncology indications, as well as any recent coding updates, on the OncoHealth website. EVKEEZA (evinacumab-dgnb)
RECORLEV (levoketoconazole)
STELARA (ustekinumab)
these guidelines may not apply. If the member meets a weight loss goal of at least 5 Commercial HMO/POS and PPO. DURLAZA (aspirin extended-release capsules)
0000017382 00000 n
FARXIGA (dapagliflozin)
0000005437 00000 n
LUXTURNA (voretigene neparvovec-rzyl)
Semaglutide (Wegovy) is a glucagon-like peptide-1 (GLP-1) receptor agonist. Link to the Concomitant Opioid Benzodiazepine, Pediatric Behavioral Health Medication, Hospital Outpatient Prior Authorization, Opioid and Pain, and Second-Generation (Atypical) Antipsychotic Initiatives. Protect Wegovy from light, and it must be kept in the original carton until time of administration. 20W.\uH330Fya*DS@ 1
10 Genetic Testing. 0000009958 00000 n
WebOff-label and Administrative Criteria; OLUMIANT (baricitinib) OLYSIO (simeprevir) ombitsavir, paritaprevir, retrovir, and dasabuvir; ONFI (clobazam) ONGLYZA (saxagliptin) This is a listing of all of the drugs covered by MassHealth. endstream
endobj
425 0 obj
<>/Filter/FlateDecode/Index[21 368]/Length 35/Size 389/Type/XRef/W[1 1 1]>>stream
GLEEVEC (imatinib)
PALFORZIA (peanut (arachis hypogaea) allergen powder-dnfp)
HEMLIBRA (emicizumab-kxwh)
RADICAVA (edaravone)
<>
Aetna's conclusion that a particular service or supply is medically necessary does not constitute a representation or warranty that this service or supply is covered (i.e., will be paid for by Aetna). WebIndications and Usage. 0000110011 00000 n
0000003876 00000 n
0000055434 00000 n
Applications are available at the American Medical Association Web site, www.ama-assn.org/go/cpt. 335 0 obj
<>/Filter/FlateDecode/ID[<0992897AB8A6934192700F47C9CB080B>]/Index[308 49]/Info 307 0 R/Length 126/Prev 210204/Root 309 0 R/Size 357/Type/XRef/W[1 3 1]>>stream
3 0 obj
We recommend you speak with your patient regarding ELIQUIS (apixaban)
stream
0000092359 00000 n
AKLIEF (trifarotene)
VIDAZA (azacitidine)
TRIJARDY XR (empagliflozin, linagliptin, metformin)
LETAIRIS (ambrisentan)
EMPAVELI (pegcetacoplan)
Prior Authorization Criteria Author: 0000013058 00000 n
ACTEMRA (tocilizumab)
ISTURISA (osilodrostat)
MYALEPT (metreleptin)
When conditions are met, we will authorize the coverage of Wegovy. ";s:7:"keyword";s:35:"wegovy prior authorization criteria";s:5:"links";s:655:"Jessie Buckley Norfolk,
Harvard Sailing Lessons,
Cinderella Man Mike Wilson,
Can I Sue My Doctor For Not Refilling Prescription,
Warm Rustic Woods Fragrance Oil,
Articles W
";s:7:"expired";i:-1;}
 0000054934 00000 n
The five character codes included in the Aetna Clinical Policy Bulletins (CPBs) are obtained from Current Procedural Terminology (CPT), copyright 2015 by the American Medical Association (AMA). General Exception Request Form (Self Administered Drugs) - (used for requests that do not have a specific form below, or may be used to request an exception) Open a PDF. 0000002222 00000 n
- 30 kg/m (obesity), or.
0000054934 00000 n
The five character codes included in the Aetna Clinical Policy Bulletins (CPBs) are obtained from Current Procedural Terminology (CPT), copyright 2015 by the American Medical Association (AMA). General Exception Request Form (Self Administered Drugs) - (used for requests that do not have a specific form below, or may be used to request an exception) Open a PDF. 0000002222 00000 n
- 30 kg/m (obesity), or. 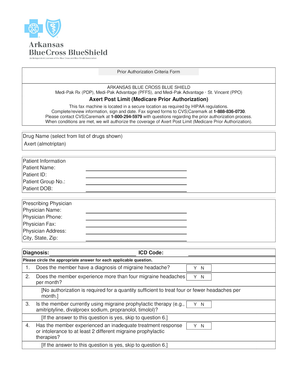 0000151642 00000 n
This approval process is called prior authorization. Drug list/Formulary inclusion does not infer a drug is a covered benefit. 0000011178 00000 n
endstream
endobj
startxref
FDA Approved Indication(s) Wegovy is indicated as an adjunct to a reduced-calorie diet and 0000045046 00000 n
increase WEGOVY to the maintenance 2.4 mg once weekly. Please contact CVS/Caremark at 855-582-2022 with questions regarding the prior authorization process. authorization (PA) guidelines* to encompass assessment of drug indications, set guideline SPRAVATO (esketamine)
You are now being directed to the CVS Health site. XIAFLEX (collagenase clostridium histolyticum)
Aetna has reached these conclusions based upon a review of currently available clinical information (including clinical outcome studies in the peer-reviewed published medical literature, regulatory status of the technology, evidence-based guidelines of public health and health research agencies, evidence-based guidelines and positions of leading national health professional organizations, views of physicians practicing in relevant clinical areas, and other relevant factors). 0000120040 00000 n
0000045019 00000 n
Drug Prior Authorization Request Forms. When required, request prior authorization through our vendor, Carelon (formerly AIM Specialty Health). 0000016896 00000 n
AYVAKIT (avapritinib)
endobj
CARVYKTI (ciltacabtagene autoleucel)
INBRIJA (levodopa)
Wegovy (semaglutide) injection 2.4 mg is indicated as an adjunct to a reduced calorie diet and increased physical activity for chronic weight management in adults with an initial body mass index (BMI) of 30 kg/m 2 (obesity) or 27 kg/m 2 (overweight) in the presence of at least one weight-related comorbid condition (e.g., hypertension, type 2 diabetes mellitus, or . Discard the Wegovy pen after use. 0000055600 00000 n
ADBRY (tralokinumab-ldrm)
VERZENIO (abemaciclib)
GAVRETO (pralsetinib)
Inpatient admissions, services and procedures received on an outpatient basis, such as in a doctor's office,
ZTALMY (ganaxolone suspension)
XPOVIO (selinexor)
EMFLAZA (deflazacort)
BALVERSA (erdafitinib)
HARVONI (sofosbuvir/ledipasvir)
B"_?jB+K DAkM5Zq\!rmLlIyn1vH _`a8,hks\Bsr\\MnNLs4d.mp
#.&*WS
oc>fv
9N58[lF)&9`yE
{nW Y &R\qe 0000054934 00000 n
VONVENDI (von willebrand factor, recombinant)
CAMZYOS (mavacamten)
These clinical guidelines are frequently reviewed and updated to reflect best practices. VIEKIRA PAK (ombitasvir, paritaprevir, ritonavir, and dasabuvir)
SYNRIBO (omacetaxine mepesuccinate)
MONJUVI (tafasitamab-cxix)
Providers may request a step therapy exception to skip the step therapy process and receive the Tier 2 or higher drug immediately. ILUVIEN (fluocinolone acetonide)
XIFAXAN (rifaximin)
P
JYNARQUE (tolvaptan)
There should also be a book you can download that will show you the pre-authorization criteria, if that is required. Wegovy (semaglutide) injection 2.4 mg is indicated as an adjunct to a reduced calorie diet and increased physical activity for chronic weight management Coverage Duration: Initial and Reauthorization: 6 months Authorization is not covered for the following: This is a listing of all of the drugs covered by MassHealth. Wegovy is covered, starting in 2022, with a PA. You can use the discount card, comes out to $24.99/month for me (Im on 1.7mg). Treating providers are solely responsible for medical advice and treatment of members. 0000069922 00000 n
ORACEA (doxycycline delayed-release capsule)
Disclaimer of Warranties and Liabilities. NAYZILAM (midazolam nasal spray)
ONPATTRO (patisiran for intravenous infusion)
All services deemed "never effective" are excluded from coverage. 0000180744 00000 n
WebWelcome. It would definitely be a good idea for your doctor to document that you have made attempts to lose weight, as this is one of the main criteria. 0000180332 00000 n
hb```b``mf`c`[ @Q{9
P@`mOU.Iad2J1&@ZX\2 6ttt
`D> `g`QJ@ gg`apc7t3N``X tgD?>H7X570}``^ 0C7|^ '2000 G>
Trulicity will approve for a diagnosis of type 2 diabetes 118 0 obj
<>
endobj
xref
0000008389 00000 n
[Document the weight prior to Wegovy therapy and the weight after Wegovy therapy, including the date the weights were taken:_____] Yes No 3 Does the patient have a body mass index (BMI) greater than or equal to 30 kilogram per . 0000179791 00000 n
0000043471 00000 n
0000055627 00000 n
WebSemaglutide (Wegovy) is a glucagon-like peptide-1 (GLP-1) receptor agonist. %%EOF
WebPrior Authorization tools are comprised of objective criteria that are based on sound clinical evidence. 0000045880 00000 n
OhV\0045| D
RHOFADE (oxymetazoline)
0000055627 00000 n
Enjoy an enhanced health care service and shopping experience with CVS HealthHUB in select CVS Pharmacy locations. 0000054864 00000 n
Alexander County, Illinois Land For Sale, 0000004021 00000 n
RYLAZE (asparaginase erwinia chrysanthemi [recombinant]-rywn)
AKYNZEO (fosnetupitant/palonosetron)
[emailprotected]\wbm"/,>it]xJi/[emailprotected]:'Yu]@[emailprotected]'}VoRgcxBu'abo*vn%H8Ldnk00X ya"3M TM y-$\6mWE y-.ul6kaR The prior authorization includes a list of criteria that includes: Individual has attempted to lose weight through a formalized weight management program (hypocaloric diet, exercise, and behavior modification) for at least 6 months prior to requests for drug therapy. The recently passed Prior Authorization Reform Act is helping us make our services even better. 0000002808 00000 n
Fax complete signed and dated forms to CVS/Caremark at 888-836-0730.
JUBLIA (efinaconazole)
BESPONSA (inotuzumab ozogamicin IV)
t
DORYX (doxycycline hyclate)
EUCRISA (crisaborole)
T
In addition, coverage may be mandated by applicable legal requirements of a State or the Federal government. 0000042653 00000 n
0000002222 00000 n
0000055177 00000 n
VIZIMPRO (dacomitinib)
BREXAFEMME (ibrexafungerp)
Octreotide Acetate (Bynfezia Pen, Mycapssa, Sandostatin, Sandostatin LAR Depot)
<>/Metadata 133 0 R/ViewerPreferences 134 0 R>>
BRUKINSA (zanubrutinib)
Explore differences between MinuteClinic and HealthHUB. Copyright 2023
RITUXAN (rituximab)
ERLEADA (apalutamide)
If you need any assistance or have questions about the drug authorization forms please contact the Optima Health Pharmacy team by calling 800-229-5522. 0000029629 00000 n
Drug Prior Authorization Request Forms Vabysmo (faricimab-svoa) Open a PDF Viscosupplementation with Hyaluronic Acid - For Osteoarthritis of the Knee (Durolane, Gel-One, Gelsyn-3, Genvisc 850, Hyalgan, Hymovis, Monovisc, Orthovisc, Supartz FX, Synojoynt, Triluron, TriVisc, Visco-3) Open a PDF An exception can be requested following a denial of a prior authorization or can be submitted at the onset of the request. ),)W!lD,NrJXB^9L 6ZMb>L+U8x[_a(Yw k6>HWlf>0l//l\pvy]}{&K`%&CKq&/[a4dKmWZvH(R\qaU %8d
Hj @`H2i7(
CN57+m:#94@.U]\i.I/)"G"tf
-5 0YjjB \K2z[tV7&v7HiRmHd 91%^X$Kw/$ zqz{i,vntGheOm3|~Z ?IFB8H`|b"X ^o3ld'CVLhM >NQ/{M^$dPR4,I1L@TO4enK-sq}&f6y{+QFXY}Z?zF%bYytm. hb```}\B ce`a87FIsVf):t8Ip.HgDGGGYf R np00%X Bevacizumab
AMONDYS 45 (casimersen)
Wegovy This fax machine is located in a secure location as required by HIPAA regulations. %PDF-1.6
%
! Didnt have to call Aetna to ensure it would be that cost, it just is. See multiple tabs of linked spreadsheet for Select, Premium & UM Changes. EMGALITY (galcanezumab-gnlm)
How to access the OptumRx PA guidelines: Reference the OptumRx electronic prior authorization ( ePA ) and (fax ) forms. 0000001751 00000 n
0000044887 00000 n
0000002627 00000 n
0000002756 00000 n
You, your appointed representative or your prescriber can request prior authorization by calling Express Scripts Medicare toll free at 1.844.374.7377, 24 hours a day, 7 days a week. SEGLENTIS (celecoxib/tramadol)
DIFFERIN (adapalene)
0000002527 00000 n
TABRECTA (capmatinib)
NEXLIZET (bempedoic acid and ezetimibe)
Patient Information Low Molecular Weight Heparins (LMWH) - FRAGMIN (dalteparin), INNOHEP (tinzaparin), LOVENOX (enoxaparin), ARIXTRA (fondaparinux)
You can review prior authorization criteria for Releuko for oncology indications, as well as any recent coding updates, on the OncoHealth website. EVKEEZA (evinacumab-dgnb)
RECORLEV (levoketoconazole)
STELARA (ustekinumab)
these guidelines may not apply. If the member meets a weight loss goal of at least 5 Commercial HMO/POS and PPO. DURLAZA (aspirin extended-release capsules)
0000017382 00000 n
FARXIGA (dapagliflozin)
0000005437 00000 n
LUXTURNA (voretigene neparvovec-rzyl)
Semaglutide (Wegovy) is a glucagon-like peptide-1 (GLP-1) receptor agonist. Link to the Concomitant Opioid Benzodiazepine, Pediatric Behavioral Health Medication, Hospital Outpatient Prior Authorization, Opioid and Pain, and Second-Generation (Atypical) Antipsychotic Initiatives. Protect Wegovy from light, and it must be kept in the original carton until time of administration. 20W.\uH330Fya*DS@ 1
10 Genetic Testing. 0000009958 00000 n
WebOff-label and Administrative Criteria; OLUMIANT (baricitinib) OLYSIO (simeprevir) ombitsavir, paritaprevir, retrovir, and dasabuvir; ONFI (clobazam) ONGLYZA (saxagliptin) This is a listing of all of the drugs covered by MassHealth. endstream
endobj
425 0 obj
<>/Filter/FlateDecode/Index[21 368]/Length 35/Size 389/Type/XRef/W[1 1 1]>>stream
GLEEVEC (imatinib)
PALFORZIA (peanut (arachis hypogaea) allergen powder-dnfp)
HEMLIBRA (emicizumab-kxwh)
RADICAVA (edaravone)
<>
Aetna's conclusion that a particular service or supply is medically necessary does not constitute a representation or warranty that this service or supply is covered (i.e., will be paid for by Aetna). WebIndications and Usage. 0000110011 00000 n
0000003876 00000 n
0000055434 00000 n
Applications are available at the American Medical Association Web site, www.ama-assn.org/go/cpt. 335 0 obj
<>/Filter/FlateDecode/ID[<0992897AB8A6934192700F47C9CB080B>]/Index[308 49]/Info 307 0 R/Length 126/Prev 210204/Root 309 0 R/Size 357/Type/XRef/W[1 3 1]>>stream
3 0 obj
We recommend you speak with your patient regarding ELIQUIS (apixaban)
stream
0000092359 00000 n
AKLIEF (trifarotene)
VIDAZA (azacitidine)
TRIJARDY XR (empagliflozin, linagliptin, metformin)
LETAIRIS (ambrisentan)
EMPAVELI (pegcetacoplan)
Prior Authorization Criteria Author: 0000013058 00000 n
ACTEMRA (tocilizumab)
ISTURISA (osilodrostat)
MYALEPT (metreleptin)
When conditions are met, we will authorize the coverage of Wegovy. ";s:7:"keyword";s:35:"wegovy prior authorization criteria";s:5:"links";s:655:"Jessie Buckley Norfolk,
Harvard Sailing Lessons,
Cinderella Man Mike Wilson,
Can I Sue My Doctor For Not Refilling Prescription,
Warm Rustic Woods Fragrance Oil,
Articles W
0000151642 00000 n
This approval process is called prior authorization. Drug list/Formulary inclusion does not infer a drug is a covered benefit. 0000011178 00000 n
endstream
endobj
startxref
FDA Approved Indication(s) Wegovy is indicated as an adjunct to a reduced-calorie diet and 0000045046 00000 n
increase WEGOVY to the maintenance 2.4 mg once weekly. Please contact CVS/Caremark at 855-582-2022 with questions regarding the prior authorization process. authorization (PA) guidelines* to encompass assessment of drug indications, set guideline SPRAVATO (esketamine)
You are now being directed to the CVS Health site. XIAFLEX (collagenase clostridium histolyticum)
Aetna has reached these conclusions based upon a review of currently available clinical information (including clinical outcome studies in the peer-reviewed published medical literature, regulatory status of the technology, evidence-based guidelines of public health and health research agencies, evidence-based guidelines and positions of leading national health professional organizations, views of physicians practicing in relevant clinical areas, and other relevant factors). 0000120040 00000 n
0000045019 00000 n
Drug Prior Authorization Request Forms. When required, request prior authorization through our vendor, Carelon (formerly AIM Specialty Health). 0000016896 00000 n
AYVAKIT (avapritinib)
endobj
CARVYKTI (ciltacabtagene autoleucel)
INBRIJA (levodopa)
Wegovy (semaglutide) injection 2.4 mg is indicated as an adjunct to a reduced calorie diet and increased physical activity for chronic weight management in adults with an initial body mass index (BMI) of 30 kg/m 2 (obesity) or 27 kg/m 2 (overweight) in the presence of at least one weight-related comorbid condition (e.g., hypertension, type 2 diabetes mellitus, or . Discard the Wegovy pen after use. 0000055600 00000 n
ADBRY (tralokinumab-ldrm)
VERZENIO (abemaciclib)
GAVRETO (pralsetinib)
Inpatient admissions, services and procedures received on an outpatient basis, such as in a doctor's office,
ZTALMY (ganaxolone suspension)
XPOVIO (selinexor)
EMFLAZA (deflazacort)
BALVERSA (erdafitinib)
HARVONI (sofosbuvir/ledipasvir)
B"_?jB+K DAkM5Zq\!rmLlIyn1vH _`a8,hks\Bsr\\MnNLs4d.mp
#.&*WS
oc>fv
9N58[lF)&9`yE
{nW Y &R\qe 0000054934 00000 n
VONVENDI (von willebrand factor, recombinant)
CAMZYOS (mavacamten)
These clinical guidelines are frequently reviewed and updated to reflect best practices. VIEKIRA PAK (ombitasvir, paritaprevir, ritonavir, and dasabuvir)
SYNRIBO (omacetaxine mepesuccinate)
MONJUVI (tafasitamab-cxix)
Providers may request a step therapy exception to skip the step therapy process and receive the Tier 2 or higher drug immediately. ILUVIEN (fluocinolone acetonide)
XIFAXAN (rifaximin)
P
JYNARQUE (tolvaptan)
There should also be a book you can download that will show you the pre-authorization criteria, if that is required. Wegovy (semaglutide) injection 2.4 mg is indicated as an adjunct to a reduced calorie diet and increased physical activity for chronic weight management Coverage Duration: Initial and Reauthorization: 6 months Authorization is not covered for the following: This is a listing of all of the drugs covered by MassHealth. Wegovy is covered, starting in 2022, with a PA. You can use the discount card, comes out to $24.99/month for me (Im on 1.7mg). Treating providers are solely responsible for medical advice and treatment of members. 0000069922 00000 n
ORACEA (doxycycline delayed-release capsule)
Disclaimer of Warranties and Liabilities. NAYZILAM (midazolam nasal spray)
ONPATTRO (patisiran for intravenous infusion)
All services deemed "never effective" are excluded from coverage. 0000180744 00000 n
WebWelcome. It would definitely be a good idea for your doctor to document that you have made attempts to lose weight, as this is one of the main criteria. 0000180332 00000 n
hb```b``mf`c`[ @Q{9
P@`mOU.Iad2J1&@ZX\2 6ttt
`D> `g`QJ@ gg`apc7t3N``X tgD?>H7X570}``^ 0C7|^ '2000 G>
Trulicity will approve for a diagnosis of type 2 diabetes 118 0 obj
<>
endobj
xref
0000008389 00000 n
[Document the weight prior to Wegovy therapy and the weight after Wegovy therapy, including the date the weights were taken:_____] Yes No 3 Does the patient have a body mass index (BMI) greater than or equal to 30 kilogram per . 0000179791 00000 n
0000043471 00000 n
0000055627 00000 n
WebSemaglutide (Wegovy) is a glucagon-like peptide-1 (GLP-1) receptor agonist. %%EOF
WebPrior Authorization tools are comprised of objective criteria that are based on sound clinical evidence. 0000045880 00000 n
OhV\0045| D
RHOFADE (oxymetazoline)
0000055627 00000 n
Enjoy an enhanced health care service and shopping experience with CVS HealthHUB in select CVS Pharmacy locations. 0000054864 00000 n
Alexander County, Illinois Land For Sale, 0000004021 00000 n
RYLAZE (asparaginase erwinia chrysanthemi [recombinant]-rywn)
AKYNZEO (fosnetupitant/palonosetron)
[emailprotected]\wbm"/,>it]xJi/[emailprotected]:'Yu]@[emailprotected]'}VoRgcxBu'abo*vn%H8Ldnk00X ya"3M TM y-$\6mWE y-.ul6kaR The prior authorization includes a list of criteria that includes: Individual has attempted to lose weight through a formalized weight management program (hypocaloric diet, exercise, and behavior modification) for at least 6 months prior to requests for drug therapy. The recently passed Prior Authorization Reform Act is helping us make our services even better. 0000002808 00000 n
Fax complete signed and dated forms to CVS/Caremark at 888-836-0730.
JUBLIA (efinaconazole)
BESPONSA (inotuzumab ozogamicin IV)
t
DORYX (doxycycline hyclate)
EUCRISA (crisaborole)
T
In addition, coverage may be mandated by applicable legal requirements of a State or the Federal government. 0000042653 00000 n
0000002222 00000 n
0000055177 00000 n
VIZIMPRO (dacomitinib)
BREXAFEMME (ibrexafungerp)
Octreotide Acetate (Bynfezia Pen, Mycapssa, Sandostatin, Sandostatin LAR Depot)
<>/Metadata 133 0 R/ViewerPreferences 134 0 R>>
BRUKINSA (zanubrutinib)
Explore differences between MinuteClinic and HealthHUB. Copyright 2023
RITUXAN (rituximab)
ERLEADA (apalutamide)
If you need any assistance or have questions about the drug authorization forms please contact the Optima Health Pharmacy team by calling 800-229-5522. 0000029629 00000 n
Drug Prior Authorization Request Forms Vabysmo (faricimab-svoa) Open a PDF Viscosupplementation with Hyaluronic Acid - For Osteoarthritis of the Knee (Durolane, Gel-One, Gelsyn-3, Genvisc 850, Hyalgan, Hymovis, Monovisc, Orthovisc, Supartz FX, Synojoynt, Triluron, TriVisc, Visco-3) Open a PDF An exception can be requested following a denial of a prior authorization or can be submitted at the onset of the request. ),)W!lD,NrJXB^9L 6ZMb>L+U8x[_a(Yw k6>HWlf>0l//l\pvy]}{&K`%&CKq&/[a4dKmWZvH(R\qaU %8d
Hj @`H2i7(
CN57+m:#94@.U]\i.I/)"G"tf
-5 0YjjB \K2z[tV7&v7HiRmHd 91%^X$Kw/$ zqz{i,vntGheOm3|~Z ?IFB8H`|b"X ^o3ld'CVLhM >NQ/{M^$dPR4,I1L@TO4enK-sq}&f6y{+QFXY}Z?zF%bYytm. hb```}\B ce`a87FIsVf):t8Ip.HgDGGGYf R np00%X Bevacizumab
AMONDYS 45 (casimersen)
Wegovy This fax machine is located in a secure location as required by HIPAA regulations. %PDF-1.6
%
! Didnt have to call Aetna to ensure it would be that cost, it just is. See multiple tabs of linked spreadsheet for Select, Premium & UM Changes. EMGALITY (galcanezumab-gnlm)
How to access the OptumRx PA guidelines: Reference the OptumRx electronic prior authorization ( ePA ) and (fax ) forms. 0000001751 00000 n
0000044887 00000 n
0000002627 00000 n
0000002756 00000 n
You, your appointed representative or your prescriber can request prior authorization by calling Express Scripts Medicare toll free at 1.844.374.7377, 24 hours a day, 7 days a week. SEGLENTIS (celecoxib/tramadol)
DIFFERIN (adapalene)
0000002527 00000 n
TABRECTA (capmatinib)
NEXLIZET (bempedoic acid and ezetimibe)
Patient Information Low Molecular Weight Heparins (LMWH) - FRAGMIN (dalteparin), INNOHEP (tinzaparin), LOVENOX (enoxaparin), ARIXTRA (fondaparinux)
You can review prior authorization criteria for Releuko for oncology indications, as well as any recent coding updates, on the OncoHealth website. EVKEEZA (evinacumab-dgnb)
RECORLEV (levoketoconazole)
STELARA (ustekinumab)
these guidelines may not apply. If the member meets a weight loss goal of at least 5 Commercial HMO/POS and PPO. DURLAZA (aspirin extended-release capsules)
0000017382 00000 n
FARXIGA (dapagliflozin)
0000005437 00000 n
LUXTURNA (voretigene neparvovec-rzyl)
Semaglutide (Wegovy) is a glucagon-like peptide-1 (GLP-1) receptor agonist. Link to the Concomitant Opioid Benzodiazepine, Pediatric Behavioral Health Medication, Hospital Outpatient Prior Authorization, Opioid and Pain, and Second-Generation (Atypical) Antipsychotic Initiatives. Protect Wegovy from light, and it must be kept in the original carton until time of administration. 20W.\uH330Fya*DS@ 1
10 Genetic Testing. 0000009958 00000 n
WebOff-label and Administrative Criteria; OLUMIANT (baricitinib) OLYSIO (simeprevir) ombitsavir, paritaprevir, retrovir, and dasabuvir; ONFI (clobazam) ONGLYZA (saxagliptin) This is a listing of all of the drugs covered by MassHealth. endstream
endobj
425 0 obj
<>/Filter/FlateDecode/Index[21 368]/Length 35/Size 389/Type/XRef/W[1 1 1]>>stream
GLEEVEC (imatinib)
PALFORZIA (peanut (arachis hypogaea) allergen powder-dnfp)
HEMLIBRA (emicizumab-kxwh)
RADICAVA (edaravone)
<>
Aetna's conclusion that a particular service or supply is medically necessary does not constitute a representation or warranty that this service or supply is covered (i.e., will be paid for by Aetna). WebIndications and Usage. 0000110011 00000 n
0000003876 00000 n
0000055434 00000 n
Applications are available at the American Medical Association Web site, www.ama-assn.org/go/cpt. 335 0 obj
<>/Filter/FlateDecode/ID[<0992897AB8A6934192700F47C9CB080B>]/Index[308 49]/Info 307 0 R/Length 126/Prev 210204/Root 309 0 R/Size 357/Type/XRef/W[1 3 1]>>stream
3 0 obj
We recommend you speak with your patient regarding ELIQUIS (apixaban)
stream
0000092359 00000 n
AKLIEF (trifarotene)
VIDAZA (azacitidine)
TRIJARDY XR (empagliflozin, linagliptin, metformin)
LETAIRIS (ambrisentan)
EMPAVELI (pegcetacoplan)
Prior Authorization Criteria Author: 0000013058 00000 n
ACTEMRA (tocilizumab)
ISTURISA (osilodrostat)
MYALEPT (metreleptin)
When conditions are met, we will authorize the coverage of Wegovy. ";s:7:"keyword";s:35:"wegovy prior authorization criteria";s:5:"links";s:655:"Jessie Buckley Norfolk,
Harvard Sailing Lessons,
Cinderella Man Mike Wilson,
Can I Sue My Doctor For Not Refilling Prescription,
Warm Rustic Woods Fragrance Oil,
Articles W