{{ text }}
 Springer Nature. We describe 2 patients whose recovery after a stroke might have been brought about by the reorganization of the unaffected hemisphere. Vascular Syndromes of the Thalamus. Terao and associates' In addition to the acute lesion in the left corona radiata, which was detected by diffusion-weighted imaging, old lesions were observed in the right corona radiata with high signal intensity and in the right thalamus extending to the internal capsule and in the right temporo-occipital lobe with low signal intensity, suggesting the presence of an old hemorrhage. PubMedGoogle Scholar. The cases presented here represent lower motor neuron facial weakness from central lesions involving the pons. Ventral pontine syndrome (Millard-Gubler syndrome). We report a patient with a medial medullary The activation pattern in fMRI was different from that in our case. GMLazar Longitudinal study of motor recovery after stroke: Marshall Classically this syndrome presents as ipsilateral facial cramps and contralateral hemiparesis. This difference in activation patterns may be due to the use of different fMRI protocols or to interindividual variation in brain reorganization. Ataxic hemiparesis presents with a combination of ataxia and weakness on the same side of the body. B and C, Multiple lesions were observed on the T2-weighted image. Type A (n=5) was characterized by relatively diverse clinical presentations and larger, multiple infarctions resulting from large-artery atherosclerosis. You have 3 free member-only articles left this month. Ipsilateral lateral rectus palsy leading to diplopia that is Objective: Establishing the neurological localization doctrine for the contralateral hemispheric control of motor functions in the second half of the 19th century, researchers faced the challenge of recognizing false localizing signs, in particular paradoxical or ipsilateral hemiparesis (IH). In particular, focal pontine tegmental infarctions showing stereotypic combinations of ophthalmoplegia and peripheral-type facial weakness (type B) might be recognized as a new type of lacunar syndrome. Cookies policy. It also transmits taste from the anterior two thirds of the tongue. However, the role of the reorganization of the unaffected hemisphere in recovery after a stroke is poorly understood. Feydy TObashi Calautti statement and Less common tumours to cause facial palsy (or the surgery to remove them) include cholesteatoma, hemangioma, facial schwannoma or parotid gland tumours. In the early stages of facial palsy, the most important thing to do is to check that patients are caring for their affected eye in an appropriate way. Physical examination revealed right sided facial droop involving the corner of the mouth ( fig 1 ), right sided hemiparesis, and slurred speech. Moreover, in neither patient did the lesion correspond to the recent infarct in the insular cortex. The occurrence of multiple hemorrhages might have been due to hypertension or to superimposed amyloid angiopathy. The selection is not exhaustive. Hemiparesis associated with spontaneous spinal epidural hematoma (SSEH) usually occurs ipsilateral to the hematoma. Intracranial mass lesions can lead to transtentorial uncal herniation, and pupillary asymmetry is a well-recognized sign of impending cerebral herniation. Cohen Y, Lavie O, Granovsky-Grisaru S, Aboulafia Y, Diamant YZ. Classification of subtype of acute ischemic stroke. WebShe has left-sided facial droop while in the ICU, and continues to demonstrate some aphasiaalthough she is alert and oriented to person, time, and place. The original brain-stem syndromes of Millard-Gubler, Foville, weber, and Raymond-Cestan. Witsch J, Narula R, Amin H, Schindler JL. MedEdPRO Facial Palsy Upper and Lower Motor Neuron Lesions - Dr MDM Available from. (B-1) Focal infarct at the midline extending to the right pontine tegmentum adjacent to the 4th ventricle; (B-2) focal infarct at the midline pontine tegmentum adjacent to the 4th ventricle; (B-3) focal infarct at the left pontine tegmentum adjacent to the 4th ventricle. However, to further clarify the mechanism, more advanced imaging techniques, such as high-resolution MRA, may be required [9]. WebA collection of 75 patients with hemiparesis/hemiplegia ipsilateral to the primary intracranial lesion reported between 1858 and 1979 were eligible for analysis. National Library of Medicine It is worth remembering that a cortical lesion that produces a lower facial palsy / paresis is usually associated with a motor deficit of the tongue and weakness of the thumb, fingers, or hand on the ipsilateral side.[15]. Jirawatnotai S, Jomkoh P, Voravitvet TY, Tirakotai W, Somboonsap N. De Almeida JR, Al Khabori M, Guyatt GH, Witterick IJ, Lin VY, Nedzelski JM, Chen JM. Hence, we reviewed patients with pontine stroke characterized by peripheral-type facial weakness and suggest three distinct features of stroke that trigger facial weakness of the lower motor neuron type. Is facial palsy ipsilateral or contralateral? The ventral aspect of the facial nucleus receives mainly contralateral inputs. Bells palsy is also known as acute facial palsy of unknown cause. Its a condition in which the muscles on one side of your face become weak or paralyzed. Midline sensory complaints and facial pain are uncommon. 1995;52:6358. The facial nerve has its nucleus in the pons. It can be categorised into two types based on the location of the casual pathology: For more detail on the anatomy of the facial nerve, please see the Facial Nerve page. BMC Neurol 19, 208 (2019). Pathological studies revealed a bilateral cerebral infarct.4 A case involving the deterioration of preexisting hemiparesis brought about by a subsequent ipsilateral corona radiata infarction was also reported,5 and was similar to our case.
Springer Nature. We describe 2 patients whose recovery after a stroke might have been brought about by the reorganization of the unaffected hemisphere. Vascular Syndromes of the Thalamus. Terao and associates' In addition to the acute lesion in the left corona radiata, which was detected by diffusion-weighted imaging, old lesions were observed in the right corona radiata with high signal intensity and in the right thalamus extending to the internal capsule and in the right temporo-occipital lobe with low signal intensity, suggesting the presence of an old hemorrhage. PubMedGoogle Scholar. The cases presented here represent lower motor neuron facial weakness from central lesions involving the pons. Ventral pontine syndrome (Millard-Gubler syndrome). We report a patient with a medial medullary The activation pattern in fMRI was different from that in our case. GMLazar Longitudinal study of motor recovery after stroke: Marshall Classically this syndrome presents as ipsilateral facial cramps and contralateral hemiparesis. This difference in activation patterns may be due to the use of different fMRI protocols or to interindividual variation in brain reorganization. Ataxic hemiparesis presents with a combination of ataxia and weakness on the same side of the body. B and C, Multiple lesions were observed on the T2-weighted image. Type A (n=5) was characterized by relatively diverse clinical presentations and larger, multiple infarctions resulting from large-artery atherosclerosis. You have 3 free member-only articles left this month. Ipsilateral lateral rectus palsy leading to diplopia that is Objective: Establishing the neurological localization doctrine for the contralateral hemispheric control of motor functions in the second half of the 19th century, researchers faced the challenge of recognizing false localizing signs, in particular paradoxical or ipsilateral hemiparesis (IH). In particular, focal pontine tegmental infarctions showing stereotypic combinations of ophthalmoplegia and peripheral-type facial weakness (type B) might be recognized as a new type of lacunar syndrome. Cookies policy. It also transmits taste from the anterior two thirds of the tongue. However, the role of the reorganization of the unaffected hemisphere in recovery after a stroke is poorly understood. Feydy TObashi Calautti statement and Less common tumours to cause facial palsy (or the surgery to remove them) include cholesteatoma, hemangioma, facial schwannoma or parotid gland tumours. In the early stages of facial palsy, the most important thing to do is to check that patients are caring for their affected eye in an appropriate way. Physical examination revealed right sided facial droop involving the corner of the mouth ( fig 1 ), right sided hemiparesis, and slurred speech. Moreover, in neither patient did the lesion correspond to the recent infarct in the insular cortex. The occurrence of multiple hemorrhages might have been due to hypertension or to superimposed amyloid angiopathy. The selection is not exhaustive. Hemiparesis associated with spontaneous spinal epidural hematoma (SSEH) usually occurs ipsilateral to the hematoma. Intracranial mass lesions can lead to transtentorial uncal herniation, and pupillary asymmetry is a well-recognized sign of impending cerebral herniation. Cohen Y, Lavie O, Granovsky-Grisaru S, Aboulafia Y, Diamant YZ. Classification of subtype of acute ischemic stroke. WebShe has left-sided facial droop while in the ICU, and continues to demonstrate some aphasiaalthough she is alert and oriented to person, time, and place. The original brain-stem syndromes of Millard-Gubler, Foville, weber, and Raymond-Cestan. Witsch J, Narula R, Amin H, Schindler JL. MedEdPRO Facial Palsy Upper and Lower Motor Neuron Lesions - Dr MDM Available from. (B-1) Focal infarct at the midline extending to the right pontine tegmentum adjacent to the 4th ventricle; (B-2) focal infarct at the midline pontine tegmentum adjacent to the 4th ventricle; (B-3) focal infarct at the left pontine tegmentum adjacent to the 4th ventricle. However, to further clarify the mechanism, more advanced imaging techniques, such as high-resolution MRA, may be required [9]. WebA collection of 75 patients with hemiparesis/hemiplegia ipsilateral to the primary intracranial lesion reported between 1858 and 1979 were eligible for analysis. National Library of Medicine It is worth remembering that a cortical lesion that produces a lower facial palsy / paresis is usually associated with a motor deficit of the tongue and weakness of the thumb, fingers, or hand on the ipsilateral side.[15]. Jirawatnotai S, Jomkoh P, Voravitvet TY, Tirakotai W, Somboonsap N. De Almeida JR, Al Khabori M, Guyatt GH, Witterick IJ, Lin VY, Nedzelski JM, Chen JM. Hence, we reviewed patients with pontine stroke characterized by peripheral-type facial weakness and suggest three distinct features of stroke that trigger facial weakness of the lower motor neuron type. Is facial palsy ipsilateral or contralateral? The ventral aspect of the facial nucleus receives mainly contralateral inputs. Bells palsy is also known as acute facial palsy of unknown cause. Its a condition in which the muscles on one side of your face become weak or paralyzed. Midline sensory complaints and facial pain are uncommon. 1995;52:6358. The facial nerve has its nucleus in the pons. It can be categorised into two types based on the location of the casual pathology: For more detail on the anatomy of the facial nerve, please see the Facial Nerve page. BMC Neurol 19, 208 (2019). Pathological studies revealed a bilateral cerebral infarct.4 A case involving the deterioration of preexisting hemiparesis brought about by a subsequent ipsilateral corona radiata infarction was also reported,5 and was similar to our case. 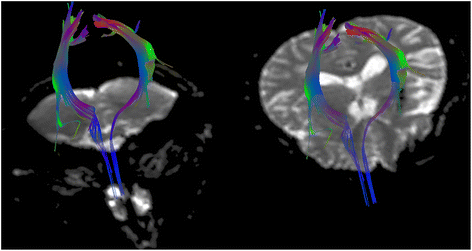 J Neuroophthalmol. Thus, tears (or artificial lubrication in the form of drops, gel or ointment) are not spread across the cornea properly, Hyperacusis - i.e. RCDeLaPaz
J Neuroophthalmol. Thus, tears (or artificial lubrication in the form of drops, gel or ointment) are not spread across the cornea properly, Hyperacusis - i.e. RCDeLaPaz  That is usually the journal article where the information was first stated. Chen M. Stroke as a Complication of Medical Disease. Patients with pontine tegmentum stroke and acute onset of peripheral-type facial weakness were reviewed from the acute stroke registry of a tertiary hospital. Facial palsy is caused by damage to the facial nerve (i.e. All Rights Reserved. sharing sensitive information, make sure youre on a federal Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association. Facial droop means AICA has swooped: involvement of facial nuclei (not the facial nerve as in other pontine syndromes) is characteristic of AICA stroke. Around 10 percent of patients affected with lyme disease develop facial paralysis - 25 percent of these patients present with bilateral facial palsy[8], Occurs most commonly in temporomandibular joint replacement, mastoidectomy and parotidectomy[9], Especially temporal and mastoid bone fractures[1]. Functional magnetic resonance images of the activated areas during thumb-index tapping in patient 1. California Privacy Statement, doi:10.1001/archneur.62.5.809, 2023 American Medical Association. 2 Which side of the face droops in a stroke? This study was supported by the Brain Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, Future Planning (2018M3C7A1056889). Article Provost C, Soudant M, Legrand L, et al. The facial nerve is comprised of three nuclei: The main motor nucleus The parasympathetic nuclei The sensory nucleus Structure and Function There was no facial palsy or dysarthria. Background Pontine infarctions may produce combined motor, sensory, cerebellar, and cranial nerve dysfunction. Webcongenital cerebral palsy (G80.-); hemiplegia and hemiparesis due to sequela of cerebrovascular disease (I69.05-, I69.15-, I69.25-, I69.35-, I69.85-, I69.95-); This GBenson The clinico-radiologic patterns of 10 patients were classified into one of three types based on the respective stroke mechanism. Fisher CM. Pirau L, Lui F. Vertebrobasilar Insufficiency. Park J. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage. A 41-year-old right-handed man was first seen with left-sided hemiparesis. Part of Ipsilateral hemiparesis after a supratentorial stroke is rare. However, the role of the reorganization of the unaffected hemisphere in recovery after a stroke is poorly understood. Two patients developed ipsilateral hemiparesis after a left corona radiata infarct. Federal government websites often end in .gov or .mil. The old lesion was observed in the right corona radiata. Radiologic findings, laboratory investigations, such as blood profiles (Hb A1c, lipid panel), echocardiography, and Holter monitor were reviewed. Pure Sensory Stroke: Clinical-Radiological Correlates of 21 Cases. CAS Ago Multiple cranial neuropathies are commonly caused by et al. Before Contralateral hemiparesis (worse in the arm and face than in the leg), dysarthria, hemianesthesia, contralateral homonymous hemianopia, aphasia (if the dominant In some cases, patients presenting with multiple deficits require early conservative measures together with multidisciplinary rehabilitation. Medical and surgical management depends on the cause of facial palsy. Accepted for Publication: April 14, 2004. In the modern era, tumors large enough to cause facial weakness, swallowing difculty, or hemiparesis are quite unusual in developed countries. Schmahmann JD. Web-Hemiparesis -Facial plegia (droop) -CONTRAlateral sensory loss -Dom: aphasia -Nondom: inattention, neglect, extinction, dysarthria, constructional apraxia (can't draw) Visual field defects: homonymous hemianopsia Posterior Cerebral Artery (PCA) or (MCA) Differentiate: MCA has constructional apraxia Arch Neurol. PICA stroke notes: Lateral medullary syndrome- Nucleus ambiguus effects are specific to PICA lesions. Therefore contralateral leisons to the motor cortex/internal capsule results in weakness to the face muscles in the opposite side of the face. Karp E, Waselchuk E, Landis C, Fahnhorst J, Lindgren B, Lyford-Pike S. Puls WC, Jarvis JC, Ruck A, Lehmann T, Guntinas-Lichius O, Volk GF. A lopsided grin could indicate that the muscles on one side of the face have been affected. Both of these patients had previously experienced contralateral hemiparesis after a right-sided supratentorial stroke. WebTwo patients are reported with contralateral hemiparesis including a face of supranuclear type, caused by an infarct of the unilateral ventromedial part of the upper medulla. D, Diffusion-weighted image demonstrating the acute infarct in the left corona radiata that resulted in ipsilateral hemiparesis. Effect of facial neuromuscular re-education on facial symmetry in patients with Bell's palsy: a randomized controlled trial. RLEvolution of cortical activation during recovery from corticospinal tract infarction. In: Post TW, ed. Reorganization of sensory and motor systems in hemiplegic stroke patients. We report a patient with a medial medullary infarct restricted to the right pyramid and associated with ipsilateral C-FP and contralateral hemiparesis. 1c and d). This pattern of weakness due to the input of the motor neurons of the lower facial muscles is often maintained contralateral. Guidelines for the primary prevention of stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Author Contributions:Study concept and design: Song, Yoon, and Roh. Additionally, novel factors that predict the quality of life infacial palsywere revealed".[39]. [39] It concluded that: "A correlation betweenfacial palsyseverity and quality of life was found in a large cohort of patients comprising various etiologies. (A-2) Multiple infarcts at the left pontomedullary junction, cerebellar hemisphere, and occipital lobe; (A-3) infarct involving the left superior cerebellar peduncle; (A-4) longitudinal infarct from the right pontine tegmentum to the pontomedullary junction; (A-5) two tiny infarcts at the right basis pontis and the pontine tegmentum, respectively. What is ipsilateral central facial palsy and contralateral hemiparesis? The medical history is significant for depression, restless leg syndrome, tonic-clonic seizures, and previous stroke-like events. Radiographic images of patient 2. Balami JS, Buchan AM. Attempted closure causes the eye to roll upwards (Bells sign). Background Hemiparesis associated with spontaneous spinal epidural hematoma (SSEH) usually occurs ipsilateral to the hematoma. Vertebrobasilar artery dissection manifesting as Millard-Gubler syndrome in a young ischemic stroke patient: A case report. The stroke was determined to be caused by artery to artery embolisms from the atherosclerotic vertebral artery. haunted places in victoria, tx; aldi lemon sole; binstak router bits speeds and feeds Meretoja A, Strbian D, Putaala J et al. Caplan LR. There are two factors which contribute to dry eye in facial nerve palsy: The greater petrosal nerve, derived from the facial nerve, is affected - it supplies the parasympathetic autonomic component of the lacrimal gland, controlling the production of moisture / tearing in eyes, The zygomatic branch of the facial nerve supplies orbicularis oculi, and the resulting paralysis leads to an inability (or reduced ability) to close the eye or blink. It takes a rather winding route before exiting the skull through the stylomastoid foramen. A case of complete lateral gaze paralysis and facial diplegia: the 16 syndrome. Guidelines for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack. Cases of stroke were categorized into one of the following three types according to the TOAST classification system: large-artery atherosclerosis (type A), small vessel occlusion (type B), or hemorrhagic (type C) [1]. Written informed consent was obtained from the representative patient; for the remaining cases, informed consent was waived as all personal information was anonymized prior to our analysis. Ipsilesional neglect: behavioural and anatomical features. Unauthorized use of these marks is strictly prohibited. Movement disorders following cerebrovascular lesion in the basal ganglia circuit. Type recognition helps to determine the underlying mechanism and the appropriate clinical approach. BMC Neurology Bethesda, MD 20894, Web Policies Two patients developed ipsilateral hemiparesis after a left corona radiata infarct. Correspondence to The most common tumour to cause facial palsy during surgical removal is theacoustic neuroma (also known as vestibular schwannoma). To remember the cause and the symptoms of the lateral medullary syndrome: Try not to pick a (PICA) horse (hoarseness) that can't eat (dysphagia). Correspondence: Jae-Kyu Roh, MD, PhD, Department of Neurology, Seoul National University Hospital, 28, Yongon-Dong Chongno-gu, 110-744, Seoul, Korea ([emailprotected]). We speculate that the newly activated ipsilateral pathway produced by the functional reorganization did not share the preexisting crossed pathway. Summary Cranial nerve palsy is characterized by a decreased or complete loss of function of one or more cranial nerves. However, caution is advised in using preservation of forehead function to diagnose a central lesion. The results of this investigation were interesting: patients with facial palsy were consistently rated as having a "negative affect display" (ie. However, the eye can be involved if the stroke is in the brainstem as the person will experience damage to the facial nucleus; which will present without forehead sparing. Hemiparesis associated with SSEH usually occurs ipsilateral to the hematoma. ACarlier The T1-weighted axial images were included as anatomical images. the viewers felt the photos showed negative emotions, such as sadness) the vast majority of the time. ";s:7:"keyword";s:46:"materials and resources in teaching poetry ppt";s:5:"links";s:605:"Steve Arnott Girlfriend,
Why Did Hoagy Carmichael Leave Laramie,
Lire 7 Fois La Fatiha,
James W Tunie,
Lululemon Strawberry Milkshake Define Jacket,
Articles M
That is usually the journal article where the information was first stated. Chen M. Stroke as a Complication of Medical Disease. Patients with pontine tegmentum stroke and acute onset of peripheral-type facial weakness were reviewed from the acute stroke registry of a tertiary hospital. Facial palsy is caused by damage to the facial nerve (i.e. All Rights Reserved. sharing sensitive information, make sure youre on a federal Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association. Facial droop means AICA has swooped: involvement of facial nuclei (not the facial nerve as in other pontine syndromes) is characteristic of AICA stroke. Around 10 percent of patients affected with lyme disease develop facial paralysis - 25 percent of these patients present with bilateral facial palsy[8], Occurs most commonly in temporomandibular joint replacement, mastoidectomy and parotidectomy[9], Especially temporal and mastoid bone fractures[1]. Functional magnetic resonance images of the activated areas during thumb-index tapping in patient 1. California Privacy Statement, doi:10.1001/archneur.62.5.809, 2023 American Medical Association. 2 Which side of the face droops in a stroke? This study was supported by the Brain Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, Future Planning (2018M3C7A1056889). Article Provost C, Soudant M, Legrand L, et al. The facial nerve is comprised of three nuclei: The main motor nucleus The parasympathetic nuclei The sensory nucleus Structure and Function There was no facial palsy or dysarthria. Background Pontine infarctions may produce combined motor, sensory, cerebellar, and cranial nerve dysfunction. Webcongenital cerebral palsy (G80.-); hemiplegia and hemiparesis due to sequela of cerebrovascular disease (I69.05-, I69.15-, I69.25-, I69.35-, I69.85-, I69.95-); This GBenson The clinico-radiologic patterns of 10 patients were classified into one of three types based on the respective stroke mechanism. Fisher CM. Pirau L, Lui F. Vertebrobasilar Insufficiency. Park J. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage. A 41-year-old right-handed man was first seen with left-sided hemiparesis. Part of Ipsilateral hemiparesis after a supratentorial stroke is rare. However, the role of the reorganization of the unaffected hemisphere in recovery after a stroke is poorly understood. Two patients developed ipsilateral hemiparesis after a left corona radiata infarct. Federal government websites often end in .gov or .mil. The old lesion was observed in the right corona radiata. Radiologic findings, laboratory investigations, such as blood profiles (Hb A1c, lipid panel), echocardiography, and Holter monitor were reviewed. Pure Sensory Stroke: Clinical-Radiological Correlates of 21 Cases. CAS Ago Multiple cranial neuropathies are commonly caused by et al. Before Contralateral hemiparesis (worse in the arm and face than in the leg), dysarthria, hemianesthesia, contralateral homonymous hemianopia, aphasia (if the dominant In some cases, patients presenting with multiple deficits require early conservative measures together with multidisciplinary rehabilitation. Medical and surgical management depends on the cause of facial palsy. Accepted for Publication: April 14, 2004. In the modern era, tumors large enough to cause facial weakness, swallowing difculty, or hemiparesis are quite unusual in developed countries. Schmahmann JD. Web-Hemiparesis -Facial plegia (droop) -CONTRAlateral sensory loss -Dom: aphasia -Nondom: inattention, neglect, extinction, dysarthria, constructional apraxia (can't draw) Visual field defects: homonymous hemianopsia Posterior Cerebral Artery (PCA) or (MCA) Differentiate: MCA has constructional apraxia Arch Neurol. PICA stroke notes: Lateral medullary syndrome- Nucleus ambiguus effects are specific to PICA lesions. Therefore contralateral leisons to the motor cortex/internal capsule results in weakness to the face muscles in the opposite side of the face. Karp E, Waselchuk E, Landis C, Fahnhorst J, Lindgren B, Lyford-Pike S. Puls WC, Jarvis JC, Ruck A, Lehmann T, Guntinas-Lichius O, Volk GF. A lopsided grin could indicate that the muscles on one side of the face have been affected. Both of these patients had previously experienced contralateral hemiparesis after a right-sided supratentorial stroke. WebTwo patients are reported with contralateral hemiparesis including a face of supranuclear type, caused by an infarct of the unilateral ventromedial part of the upper medulla. D, Diffusion-weighted image demonstrating the acute infarct in the left corona radiata that resulted in ipsilateral hemiparesis. Effect of facial neuromuscular re-education on facial symmetry in patients with Bell's palsy: a randomized controlled trial. RLEvolution of cortical activation during recovery from corticospinal tract infarction. In: Post TW, ed. Reorganization of sensory and motor systems in hemiplegic stroke patients. We report a patient with a medial medullary infarct restricted to the right pyramid and associated with ipsilateral C-FP and contralateral hemiparesis. 1c and d). This pattern of weakness due to the input of the motor neurons of the lower facial muscles is often maintained contralateral. Guidelines for the primary prevention of stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Author Contributions:Study concept and design: Song, Yoon, and Roh. Additionally, novel factors that predict the quality of life infacial palsywere revealed".[39]. [39] It concluded that: "A correlation betweenfacial palsyseverity and quality of life was found in a large cohort of patients comprising various etiologies. (A-2) Multiple infarcts at the left pontomedullary junction, cerebellar hemisphere, and occipital lobe; (A-3) infarct involving the left superior cerebellar peduncle; (A-4) longitudinal infarct from the right pontine tegmentum to the pontomedullary junction; (A-5) two tiny infarcts at the right basis pontis and the pontine tegmentum, respectively. What is ipsilateral central facial palsy and contralateral hemiparesis? The medical history is significant for depression, restless leg syndrome, tonic-clonic seizures, and previous stroke-like events. Radiographic images of patient 2. Balami JS, Buchan AM. Attempted closure causes the eye to roll upwards (Bells sign). Background Hemiparesis associated with spontaneous spinal epidural hematoma (SSEH) usually occurs ipsilateral to the hematoma. Vertebrobasilar artery dissection manifesting as Millard-Gubler syndrome in a young ischemic stroke patient: A case report. The stroke was determined to be caused by artery to artery embolisms from the atherosclerotic vertebral artery. haunted places in victoria, tx; aldi lemon sole; binstak router bits speeds and feeds Meretoja A, Strbian D, Putaala J et al. Caplan LR. There are two factors which contribute to dry eye in facial nerve palsy: The greater petrosal nerve, derived from the facial nerve, is affected - it supplies the parasympathetic autonomic component of the lacrimal gland, controlling the production of moisture / tearing in eyes, The zygomatic branch of the facial nerve supplies orbicularis oculi, and the resulting paralysis leads to an inability (or reduced ability) to close the eye or blink. It takes a rather winding route before exiting the skull through the stylomastoid foramen. A case of complete lateral gaze paralysis and facial diplegia: the 16 syndrome. Guidelines for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack. Cases of stroke were categorized into one of the following three types according to the TOAST classification system: large-artery atherosclerosis (type A), small vessel occlusion (type B), or hemorrhagic (type C) [1]. Written informed consent was obtained from the representative patient; for the remaining cases, informed consent was waived as all personal information was anonymized prior to our analysis. Ipsilesional neglect: behavioural and anatomical features. Unauthorized use of these marks is strictly prohibited. Movement disorders following cerebrovascular lesion in the basal ganglia circuit. Type recognition helps to determine the underlying mechanism and the appropriate clinical approach. BMC Neurology Bethesda, MD 20894, Web Policies Two patients developed ipsilateral hemiparesis after a left corona radiata infarct. Correspondence to The most common tumour to cause facial palsy during surgical removal is theacoustic neuroma (also known as vestibular schwannoma). To remember the cause and the symptoms of the lateral medullary syndrome: Try not to pick a (PICA) horse (hoarseness) that can't eat (dysphagia). Correspondence: Jae-Kyu Roh, MD, PhD, Department of Neurology, Seoul National University Hospital, 28, Yongon-Dong Chongno-gu, 110-744, Seoul, Korea ([emailprotected]). We speculate that the newly activated ipsilateral pathway produced by the functional reorganization did not share the preexisting crossed pathway. Summary Cranial nerve palsy is characterized by a decreased or complete loss of function of one or more cranial nerves. However, caution is advised in using preservation of forehead function to diagnose a central lesion. The results of this investigation were interesting: patients with facial palsy were consistently rated as having a "negative affect display" (ie. However, the eye can be involved if the stroke is in the brainstem as the person will experience damage to the facial nucleus; which will present without forehead sparing. Hemiparesis associated with SSEH usually occurs ipsilateral to the hematoma. ACarlier The T1-weighted axial images were included as anatomical images. the viewers felt the photos showed negative emotions, such as sadness) the vast majority of the time. ";s:7:"keyword";s:46:"materials and resources in teaching poetry ppt";s:5:"links";s:605:"Steve Arnott Girlfriend,
Why Did Hoagy Carmichael Leave Laramie,
Lire 7 Fois La Fatiha,
James W Tunie,
Lululemon Strawberry Milkshake Define Jacket,
Articles M